Patient-Centered Payment
Key Elements of Patient-Centered Payment
Current approaches to value-based payment are payer-centered. Their primary focus has been to limit or reduce spending for health insurance plans, rather than to help patients receive high-quality care at the most affordable cost. Current approaches to value-based payment assess whether the average quality of care for the health plan’s members has improved or worsened, not whether each individual patient received high-quality care. Moreover, providers can be financially penalized when they treat patients with higher-than-average needs. As a result, the actions providers must take to succeed under these payment systems can be in direct conflict with doing what is best for patients.
What is needed instead is a patient-centered approach to value-based payment, one that will solve the problems in current fee-for-service payment systems without reducing access to services or the quality of care for patients.
In a Patient-Centered Payment system:
A patient is able to receive the services that will best address their specific health problems. In order for patients to receive the highest-value care, the many gaps in the services eligible for payment under current fee-for-service systems have to be filled. For example, the biggest transformation in healthcare delivery in decades was the dramatic expansion of telehealth services during the COVID-19 pandemic. None of the current value-based payment systems had supported this. It only happened because Medicare and health insurance plans began paying fees for these services for the first time. In a patient-centered payment system, providers should be paid for delivering the types of services that patients need in the way that will work best for the patient.
Each patient is assured of receiving appropriate, evidence-based care. In a patient-centered payment system, in order to be paid for delivering a service to a patient, a healthcare provider should be required to meet an appropriate standard of quality for that specific patient:
- If a desired outcome of the service is within the control of the provider, the provider should only be paid if the outcome is achieved.
- If a desired outcome is significantly affected by factors outside the control of the provider (e.g., a patient’s ability or willingness to follow a particular course of treatment), the provider should only be paid if the services that are delivered or ordered are consistent with evidence-based clinical practice guidelines (unless there are no relevant guidelines or there are good reasons to deviate from them), and if the provider monitors the desired outcomes so services can be modified for patients who are experiencing problems. If a provider cannot control whether an outcome is achieved, attempting to hold the provider accountable for the outcome is more likely to discourage the provider from treating high-need patients than it is to improve outcomes for those patients. In general, the best way for a patient to achieve a good outcome is to receive the services that evidence indicates will be most effective.
A healthcare provider receives adequate resources to support the cost of delivering services in a high-quality, efficient manner. No business can deliver a high-quality product unless it is paid enough to cover the costs of producing that product; similarly, a healthcare provider cannot be expected to deliver the kinds of services each patient needs in a high-quality way unless the payments it receives for its services are sufficient to cover the costs of doing so. Moreover, just like any business, a healthcare provider is less likely to deliver a high-quality service if it is paid more for delivering a low-quality service. In a patient-centered payment system:
- a provider’s payment should be based on what it costs to deliver high-quality care, not based on the fees paid in the past, the amount of savings that has been produced, or an arbitrary percentage of total spending.
- a provider should be paid more for patients who need more services or services that cost more to deliver.
- the patient or payer should not have to pay more because of errors and complications that the provider could have prevented.
A patient can select a provider or team based on the quality and cost of the care they deliver. Different patients have different needs and they will require different sets of services to address those needs. No one healthcare provider or health system will be the best at delivering all of the services an individual patient may need or for treating a particular health problem for all types of patients, so if patients are forced to receive services from providers in the same health system or from a “narrow network” chosen by a health insurance plan, some patients will not receive the best care possible. There is no simple measure of “value” that can be used to rank-order providers, because quality is multi-dimensional and cannot be converted into a dollar amount that is directly comparable to costs. Consequently, in a patient-centered payment system:
- providers should define in advance how much a patient or payer will have to pay for care of a patient’s specific health problem and the standard of care or outcomes the provider commits to deliver in return for that payment;
- each patient should be able to choose which provider will deliver their care based on information about both (a) what it will cost for the provider to treat the patient’s health problem and (b) the outcomes and approach to care delivery that are most important to the patient.
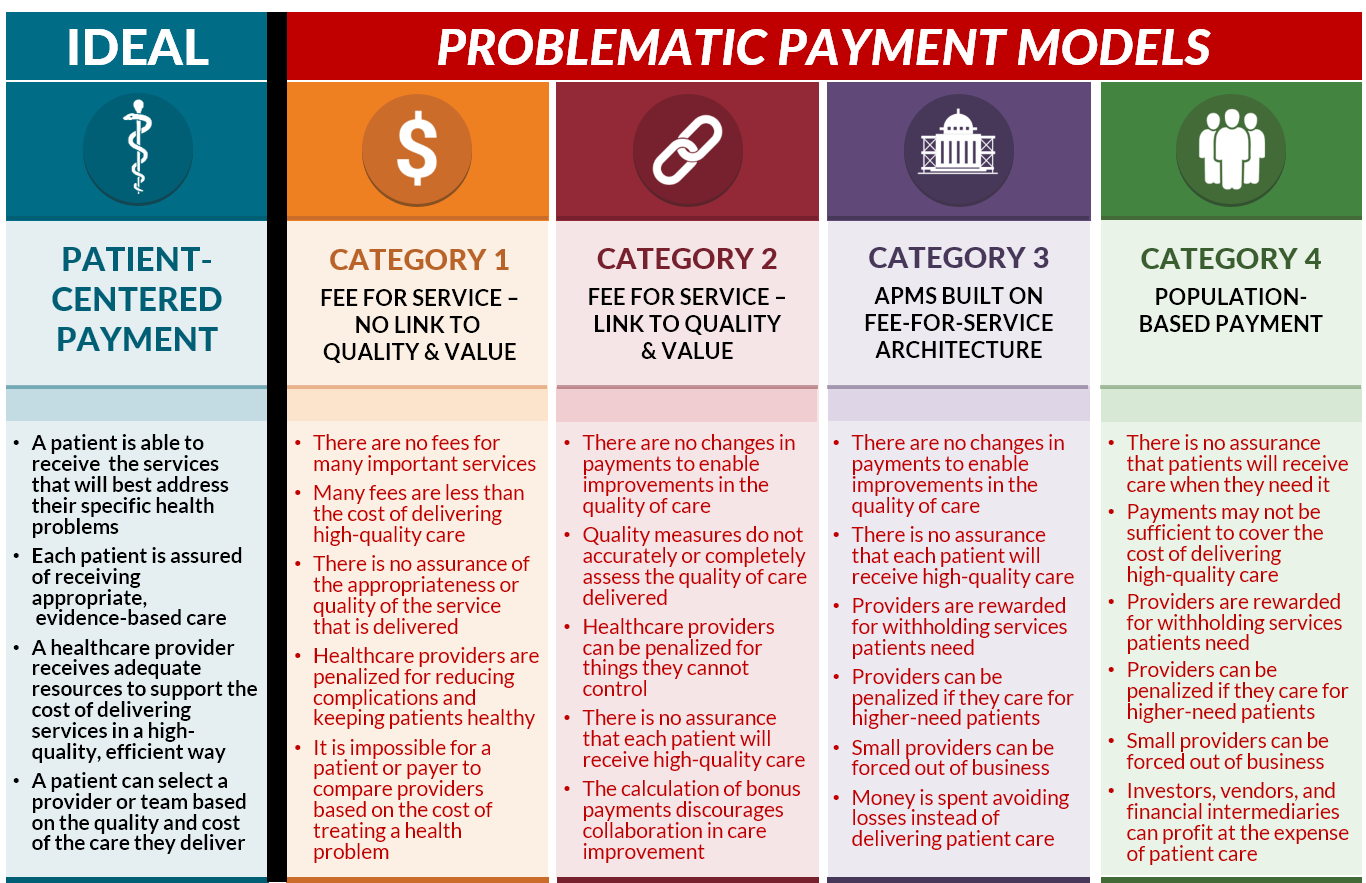
Patient-Centered Payment vs. Current Value-Based Payments
Patient-Centered Payment addresses all of the problems with current fee-for-service payment systems without causing the additional problems created by current approaches to value-based payment:
- Patient-Centered Payment would fill the gaps in current Fee for Service systems by paying adequately for the services patients need, including proactive wellness care and care management designed to help patients stay healthy and reduce avoidable services. Physicians, hospitals, and other providers would have the flexibility to deliver services in whatever manner works best for an individual patient.
- Compared to Pay for Performance programs, Patient-Centered Payment would assure that every patient receives high-quality care, not just a majority of patients, and not just the subset of patients for whom current quality measures are applicable. The provider of care would be able to deliver the services that will achieve the best outcome for each patient, and they would be accountable for doing what is feasible to achieve, not for things they cannot control.
- Compared to Shared Savings/Downside Risk programs, in a Patient-Centered Payment system there would be no reward for stinting on necessary care, nor would there be a penalty for delivering more services or more expensive services to patients who need them. Physicians, hospitals, and other providers would be paid for delivering appropriate, evidence-based services, and they would not be paid for inappropriate or poor-quality services.
- Compared to Population-Based Payment and Capitation programs, Patient-Centered Payment would provide payments that are adequate to enable providers to deliver appropriate, high-quality services to address each of their patients’ needs, including patients with acute health problems, new chronic conditions, and/or barriers to receiving services in traditional ways. Physicians and hospitals would only be paid if they actually address a patient’s needs.
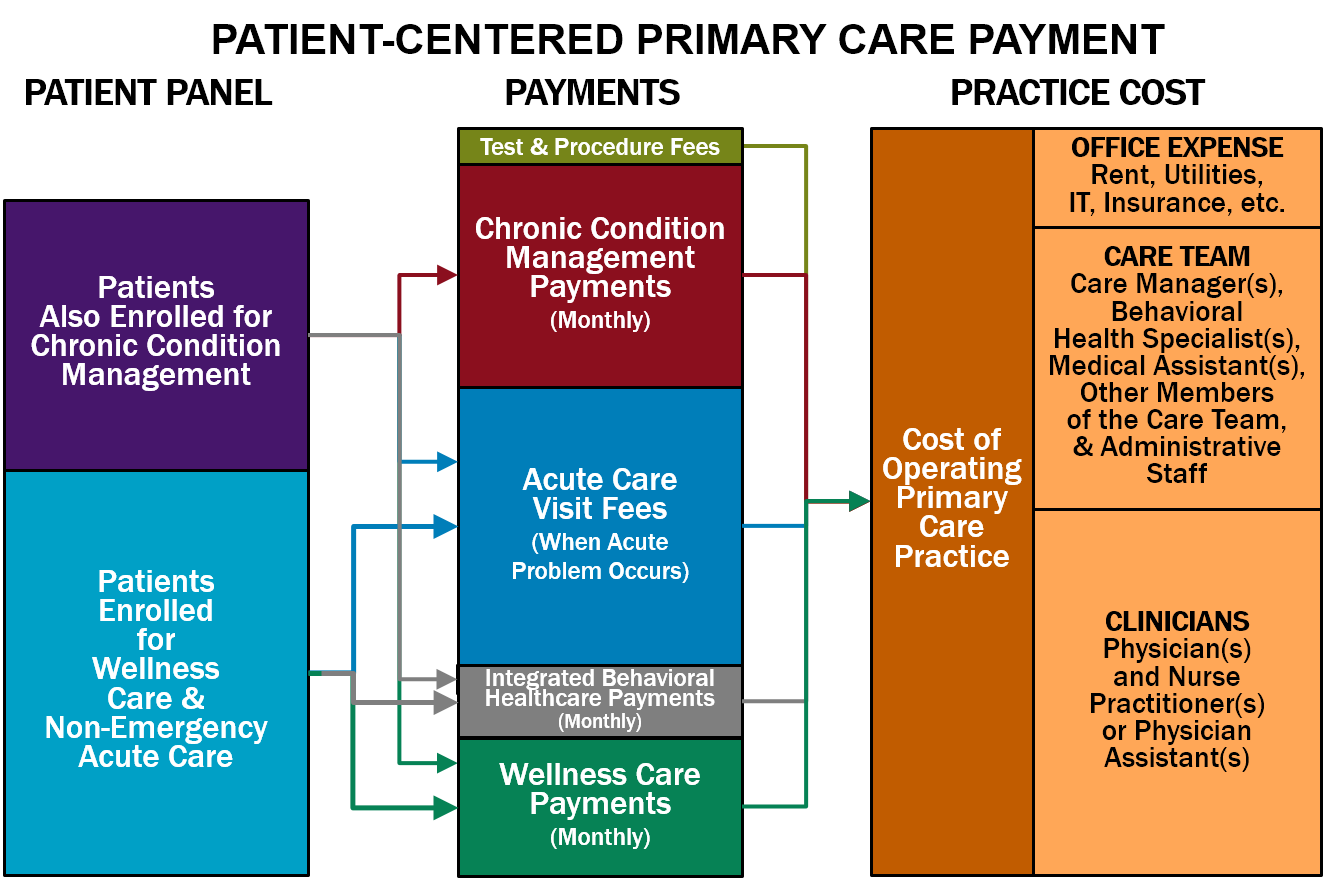
Patient-Centered Payment for Primary Care
Primary care is an essential component of a high-value healthcare system. Primary care practices deliver three important types of services to patients:
- Wellness Care. Primary care practices help patients stay healthy by educating them about what they should do to maintain and improve their health and by ensuring that patients have obtained appropriate preventive care services, such as vaccinations and cancer screenings.
- Chronic Condition Management. For patients who have one or more chronic diseases or long-term health problems, primary care practices not only prescribe appropriate treatments but also help patients understand how best to manage their condition(s) in a way that minimizes the number and severity of complications and slows the progression of the disease.
- Non-Emergency Acute Care. For patients who experience a new symptom or have an injury that does not require emergency care, the primary care practice can either diagnose and treat the problem or arrange for the patient to receive appropriate testing and treatment from other healthcare providers.
Ideally, primary care practices would also provide:
- Integrated Behavioral Health Services. Patients who have both behavioral health needs and physical health needs should be able to have them treated and managed in a coordinated way.
Neither the current fee-for-service system nor current value-based payment systems provide payments to primary care practices that are appropriately structured or adequate in size to support and sustain these services. As a result, there is a large and growing shortage of primary care physicians in the country, many primary care physicians are burning out, and most medical students don’t want to go into primary care.
In a patient-centered payment system, a primary care practice should receive adequate payments for each of these types of services in order to ensure that: (1) each patient can receive high-quality care appropriate for their specific needs, and (2) primary care practices with different types of patients receive sufficient revenues to cover the costs of the services their patients need.
Patient-Centered Primary Care Payment should consist of:
- Monthly Payments for Wellness Care. Maintaining and improving health is a continuous process that occurs throughout the year, not simply through occasional office visits. This proactive care should be supported by a monthly payment for each patient who enrolls with the primary care practice to receive wellness care. The monthly payment would support wellness care management; service-specific fees should continue to be paid for any procedures, tests, or treatments the patient needs as part of their wellness plan, such as immunizations, mammograms, colonoscopies, etc. (In some cases, these procedures, tests, and treatments may be delivered by the primary care practice, but in many cases, a specialty care provider will provide these services.)
- Monthly Payments for Chronic Condition Management. If a patient with one or more chronic conditions (such as asthma, diabetes, or hypertension) wants the primary care practice to help manage those conditions, the practice should receive an additional monthly payment for that patient in order to deliver chronic condition management services. Since continuous, proactive care is needed to reduce the severity of symptoms and prevent exacerbations of the condition, a monthly payment is necessary to support this. A higher monthly payment will be needed during the initial month following diagnosis or enrollment in order to develop the most effective treatment plan and to ensure it is effective, and a higher monthly payment will be needed for a patient with a combination of chronic conditions or other characteristics that require significantly more time and assistance. Some patients with a chronic condition will need or want to receive support from a specialty care provider, particularly patients with severe conditions and patients for whom standard treatments are not effective or have problematic side effects. Consequently, the primary care practice should only receive a monthly Chronic Condition Management Payment for a patient who explicitly enrolls with the primary care practice to receive chronic care management.
- A Fee for Diagnosis and Treatment of a Non-Emergency Acute Event. Some patients who are receiving good preventive care and chronic disease management will have accidental injuries, acute illnesses, or problematic symptoms that will require additional services from the primary care practice. Since these events will occur unpredictably, and different patients may be more susceptible to these problems than others, the primary care practice should receive an Acute Care Visit Fee when it provides diagnosis and treatment services for a new acute event. The practice should be permitted to deliver services in whatever way is most appropriate in the circumstances, including by telephone, telehealth, or an in-person visit with the physician or other practice staff. The Acute Care Visit Fee would not be paid for care of a patient experiencing an exacerbation of a chronic disease, however, since the cost of that kind of care would already be covered by the monthly payment for chronic condition management.
- Monthly Payments for Integrated Behavioral Healthcare Services. Primary care practices that deliver integrated behavioral health services to their patients need to employ or contract with staff who have training in helping patients with behavioral health needs. In order to support this, the practice should receive an additional monthly payment for each patient who is enrolled to receive wellness care from the practice.
- Fees for Individual Procedures and Tests. Many primary care practices also perform procedures such as an immunization, injection, or excision and/or perform basic laboratory tests. It is beneficial for patients to be able to receive these procedures and tests from the primary care practice if possible, rather than needing to make a separate trip to another physician or facility. Since only a subset of patients will need these procedures and tests, and since the cost of performing each of them will differ, the primary care practice should receive an additional fee when it performs a procedure or test that is adequate to cover the cost.
In order to assure that each individual patient receives appropriate, high-quality care, a primary care practice should be required to:
- Deliver Evidence-Based Care. The primary care practice should only bill and be paid for a Monthly Wellness Care Payment, Monthly Integrated Behavioral Healthcare Payment, Monthly Chronic Condition Management Payment, or Acute Care Visit Fee if the practice delivered all appropriate services to the patient during the month or acute care visit that are consistent with applicable, evidence-based Clinical Practice Guidelines (CPGs) or the practice had documented the reasons for deviation from those guidelines in the patient’s clinical record; and
- Monitor Patient Needs and Outcomes. The practice should only bill for and be paid the monthly payments if it used a Standardized Assessment, Information, and Networking Technology (SAINT) to identify and prioritize any problems the patient is experiencing and to determine whether the practice’s services are effectively addressing the patient’s needs. For example, How’s Your Health is a SAINT specifically designed for primary care that is used by many small practices.
The payment amounts should be based on the estimated cost for a primary care practice to deliver each category of service, considering the amount of time needed to deliver evidence-based services, the types of personnel who are most appropriate to deliver the services and their compensation levels, and non-personnel costs such as information systems, equipment, and space. The following amounts would likely be needed by most primary care practices to deliver high-quality care:
- a $7.40 Monthly Wellness Care Management Payment for each patient enrolled for wellness care.
- a $4.25 Monthly Integrated Behavioral Healthcare Payment if the practice offers integrated behavioral healthcare services.
- a $30.60 Monthly Chronic Condition Management Payment for each patient with a chronic condition who is enrolled with the practice for chronic condition care. A higher amount ($54.60 per month) would be needed for patients with complex conditions.
- a $141 Acute Visit Fee for a patient who has a new acute problem (not related to a chronic condition).
For patients with insurance, cost-sharing amounts should be established that enable and encourage patients to use the primary care practice:
- A modest co-payment for acute care visits;
- No cost-sharing for wellness care; and
- No cost-sharing for chronic condition management.
More Details on Patient-Centered Primary Care Payment
Patient-Centered Payment for Specialty Care
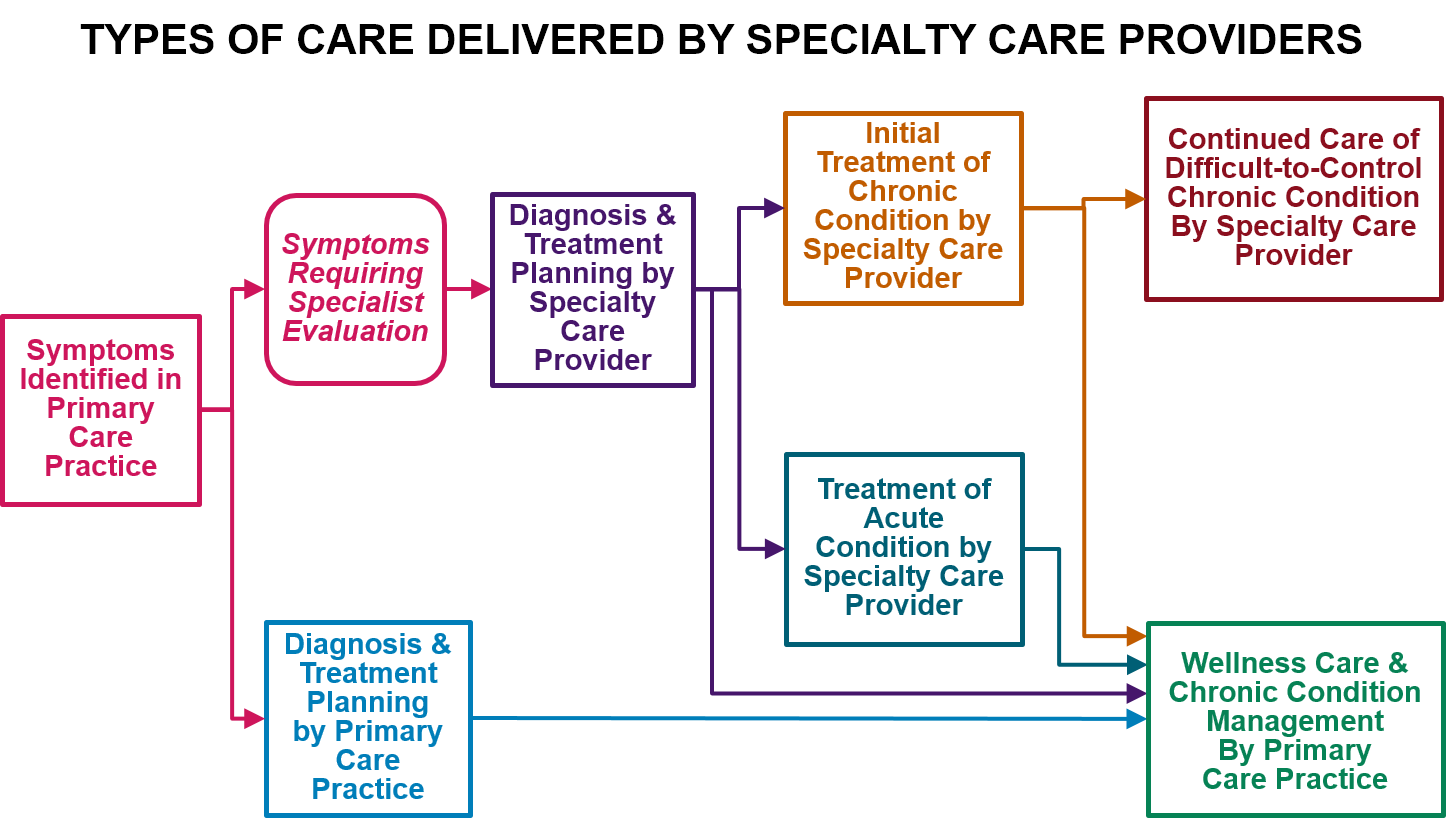
Many patients have health problems that require specialized expertise to diagnose or treat. Specialty care providers deliver three types of services that complement the work that primary care practices do:
- Diagnosis and Treatment Planning. In some cases, it is difficult to determine the cause of a patient’s symptoms without specialized training and experience. An inaccurate diagnosis can lead to unnecessary or harmful treatment for a non-existent problem and/or failure to properly treat the real problem. In addition, many patients receive unnecessary tests and/or unnecessarily expensive tests to rule out unlikely diagnoses. In some cases, these tests can lead to false positive results that contribute to inaccurate diagnoses and unnecessary treatments.
- Management of Chronic Conditions. Although many chronic conditions can be managed effectively by a primary care practice, some patients with a chronic condition will need or want to receive support from a specialty care provider, particularly patients with severe conditions (including serious behavioral health conditions) and patients for whom standard treatments are not effective or have problematic side effects. In addition, some patients with a chronic condition may need to temporarily receive treatment and proactive management services for that condition from a specialty practice rather than the primary care practice, such as when the patient experiences an acute condition that complicates management of the chronic condition (e.g., the patient becomes pregnant and the medications she had been taking for the chronic condition are problematic during pregnancy).
- Treatment of Serious Acute Conditions. Treatments and procedures for serious acute conditions may require not only special expertise, special equipment, or special facilities to perform, but multiple providers may need to contribute components of the necessary care. For example, a patient who needs surgery will require the services of a surgeon, an anesthesiologist, a hospital, and potentially other physicians and post-acute care providers in order to achieve the best outcome. All of these providers have to work together as a team if the patient is to receive care in the most effective, efficient way.
Many current value-based payment systems try to discourage the use of specialty care regardless of whether patients need it or not, or they penalize the use of expensive components of specialty care (e.g., drugs or rehabilitation) in ways that can be harmful to the patients who need those types of services. There are very few value-based payment systems specifically designed to support high-quality specialty care, particularly ambulatory specialty care.
In a patient-centered payment system, payments should enable patients to receive services that require specialized expertise, and the payments should encourage a team-based approach to specialty care delivery when multiple providers are involved. No one payment method can support all types of care for all patients.
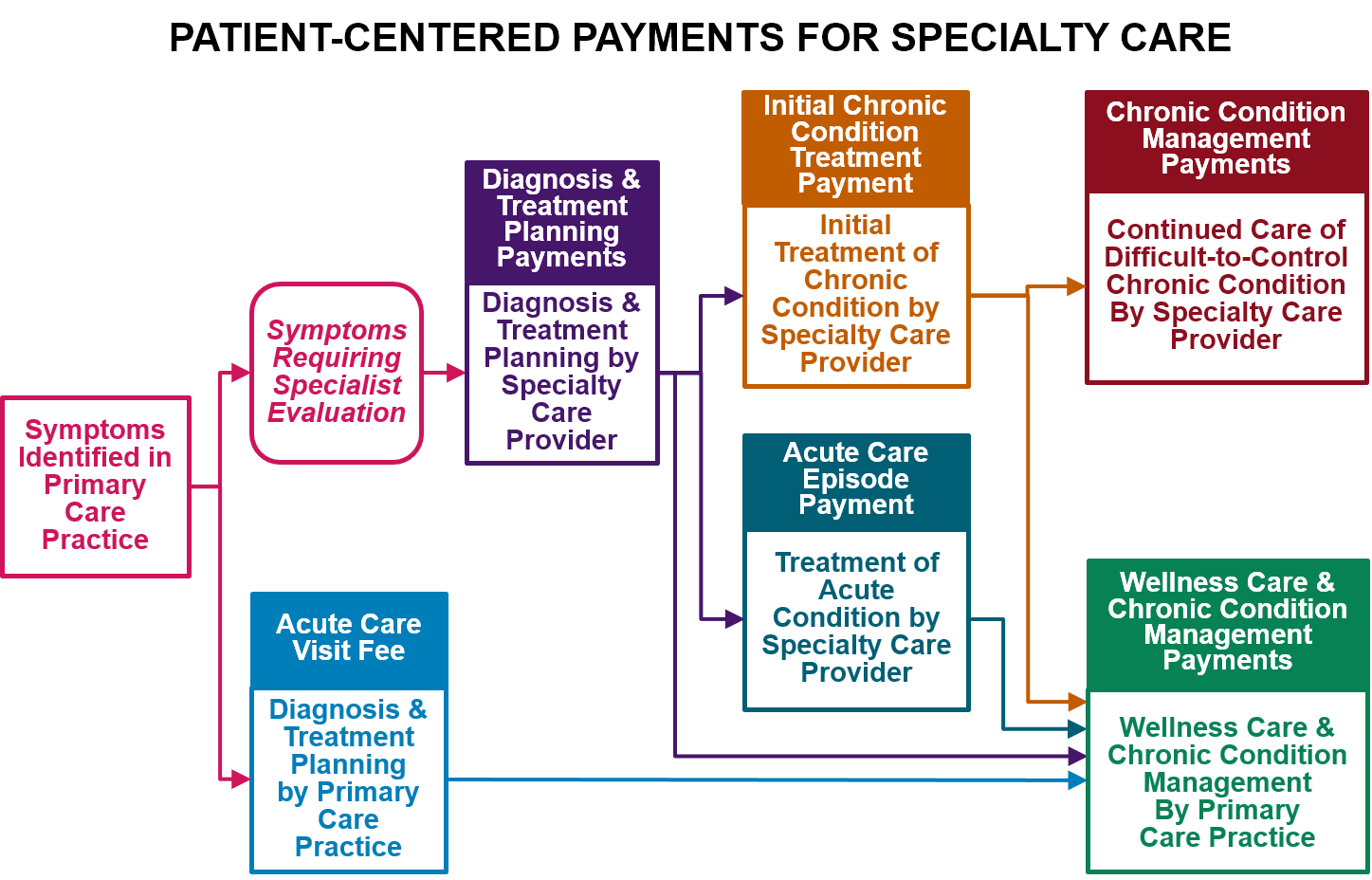
Patient-Centered Payment for Specialty Care will require four different types of payment:
- Payments for Diagnosis and Treatment Planning. A physician (or team of physicians) with expertise in diagnosing the cause of a specific symptom or set of symptoms should receive a one-time Diagnosis Payment to support the time involved in determining an appropriate diagnosis. In cases where the same symptoms could result from very different kinds of problems, separate payments to two or more specialty providers may be necessary. If the patient is diagnosed with a specific health problem, there should be an additional Treatment Planning Payment to support the time needed to work with the patient to plan an appropriate treatment. If the patient’s symptoms can be diagnosed by a primary care practice, the Acute Care Visit Fee would serve both of these functions, but if the primary care physician determines that a patient needs to see a specialty provider for diagnosis and/or treatment planning, these separate payments would support the specialty provider’s services.
- An Episode Payment for Treatment of Common Acute Conditions. For common acute conditions where there is an evidence-based protocol for treatment, such as many types of surgeries for patients with no unusual characteristics, the team of providers delivering the treatment should receive an Acute Condition Episode Payment, i.e., a single “bundled” payment for all of the services that all of the providers deliver in order for the patient to receive all components of appropriate, evidence-based care for the condition. The amount of the payment should be based on the cost of the specific services that need to be delivered.
- Monthly Payments for Management of Chronic and Extended Acute Conditions. Similar to chronic conditions managed by primary care practices, if a patient enrolls with a specialty provider for ongoing assistance in treating and managing a chronic condition, that provider should receive a Monthly Chronic Condition Management Payment for that patient to support delivery of appropriate chronic condition management services. Since continuous, proactive care is needed to reduce the severity of symptoms and prevent exacerbations of the condition, a monthly payment is necessary to support this. Monthly payments are also appropriate for patients with an acute condition that will require focused treatment or management over an extended period of time, but where the exact length of treatment is uncertain or the intensity of treatment may vary from month to month, such as patients with cancer and women who are pregnant. Higher monthly payments will be needed for patients with a combination of chronic conditions or other characteristics that require significantly more time and assistance, and higher payments will be needed when treatment first begins.
- Payments for Coordinated Treatment of Uncommon or Complex Conditions. For patients who have an uncommon acute or chronic condition or who have other characteristics that require special approaches to treatment, it may be either impossible or inappropriate to prospectively define an episode payment or monthly payment for their treatment. In these cases, the members of the provider team treating the patient should receive (a) fees for each of the individual services they deliver, and (b) a Treatment Coordination Payment to ensure that all of the services are effectively coordinated and that quality standards are met.
In order to assure that each individual patient receives appropriate, high-quality specialty care, a specialty provider or team of providers should be required to:
- Deliver Evidence-Based Care. The specialty provider team should only bill and be paid for a Diagnosis or Treatment Planning Payment, a Monthly Chronic Condition Management Payment, an Acute Condition Episode Payment, or Treatment Coordination Payment if the patient had received all services that are consistent with applicable, evidence-based Clinical Practice Guidelines (CPGs) or the provider had documented the reasons for deviation from those guidelines in the patient’s clinical record.
- Monitor Patient Outcomes. The provider should only bill for and be paid for services if it used a Standardized Assessment, Information, and Networking Technology (SAINT) to monitor whether the treatments and services delivered are achieving the desired outcomes.
- Achieve Outcomes Within the Control of the Provider. If a specific outcome can be defined that is desirable for the patient, feasible to achieve, and under the control of the provider or team of providers treating or managing the patient’s health condition, then the provider team should also be held accountable for achieving that outcome in order to receive payment for their services. However, this will generally only be possible for patients with a common chronic or acute condition and no special characteristics.
- Contribute Information to a Clinical Data Registry. Data on outcomes achieved for patients are essential for developing the evidence necessary to fill the gaps in current clinical practice guidelines and to update the guidelines as new treatments and approaches to care delivery are developed. Participation in a Clinical Data Registry enables information on services and outcomes from multiple providers to be assembled in a way that supports analysis and research on the effectiveness of different approaches to diagnosis and treatment for patients with specific characteristics.
The amounts of payments should be based on the estimated cost for a specialty provider or team to deliver the care during a month or episode of care, considering the amount of time needed to deliver evidence-based services, the types of personnel and facilities that are most appropriate to deliver the services, the cost of drugs and medical devices used for treatment or condition monitoring, the cost of collecting outcome data and participating in a clinical data registry, and other costs such as equipment, utilities, and space.
For patients with insurance, cost-sharing amounts should be designed to enable and encourage patients to receive services that improve outcomes and to use providers that deliver good outcomes at a lower cost.
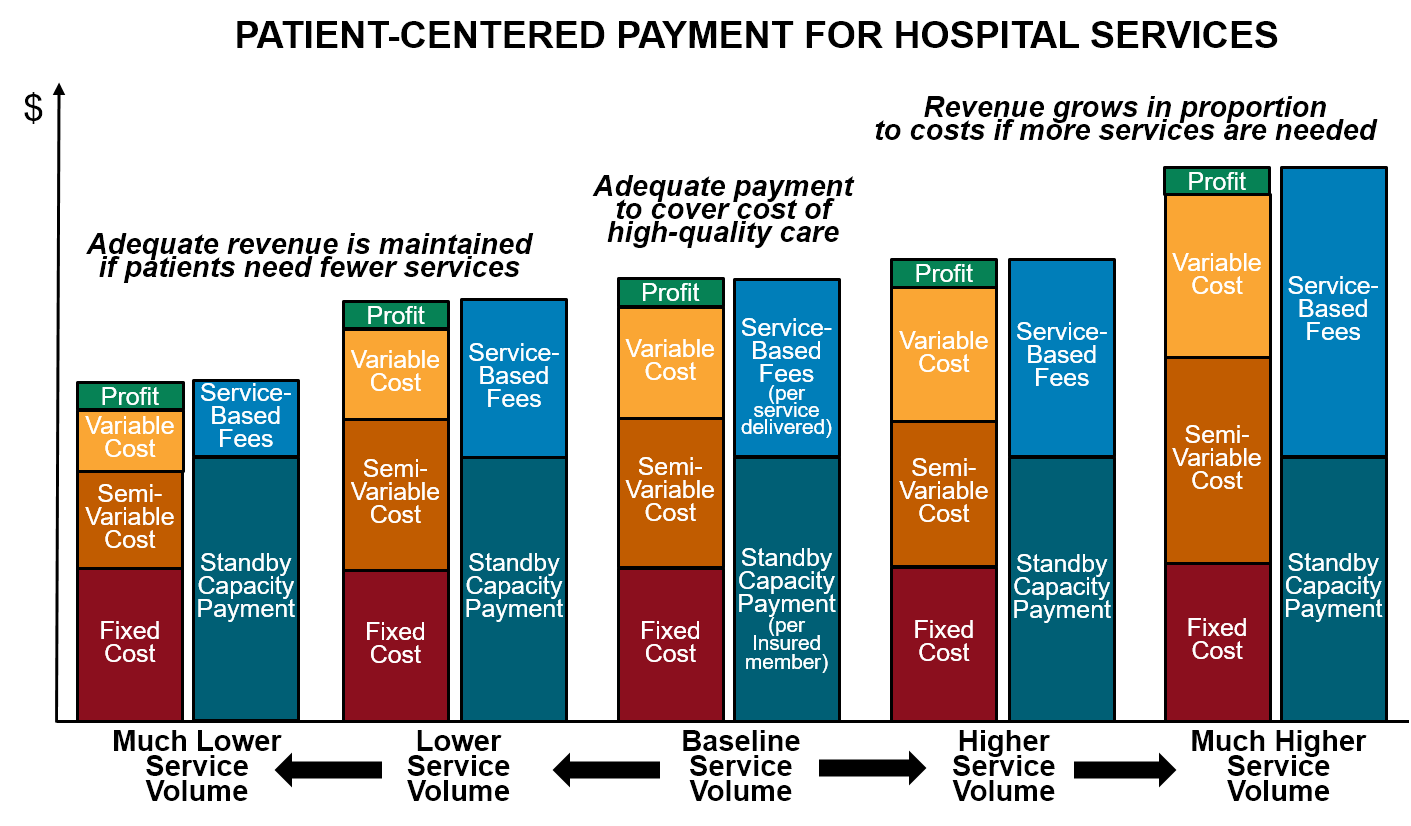
Standby Capacity Payment for Essential Hospital Services
Most current value-based payment systems are specifically intended to reduce the frequency with which patients receive hospital services, since research has shown that many of the biggest opportunities to improve quality and reduce spending involve reducing avoidable hospital admissions and delivering services in ambulatory care settings or patients’ homes. Success under these value-based payment models means hospitals will receive lower revenues, but none of the current payment models attempt to ensure that hospitals will continue to receive enough revenues to support high-quality care for the smaller number of patients who will still need hospital care:
- There is a significant fixed cost associated with each hospital service line, which means the average cost of delivering an individual service will be higher when fewer services are delivered. Because most current value-based payment systems continue to pay for individual services using standard fee-for-service payments, and the fees are typically based on the average cost of services at current volumes of service delivery, a reduction in the number of services delivered will cause a hospital’s revenues to decrease more than its costs will decrease, particularly in the short run, causing a financial loss.
- Moreover, the patients who will continue to need care in a hospital will be the most complex patients, who are more expensive on average to care for, causing the financial loss to be even greater.
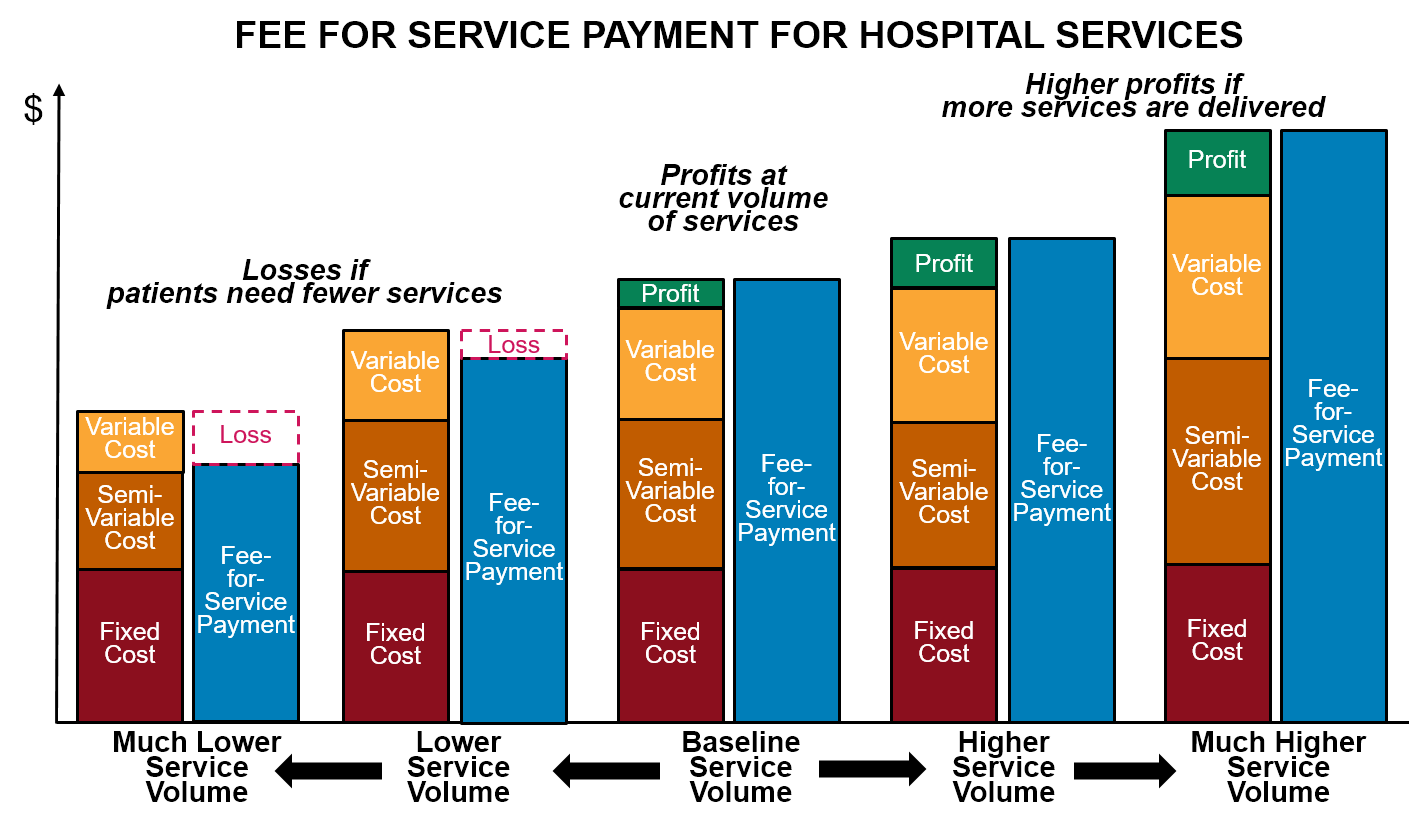
These financial losses could reduce access to hospital services for the patients who still need them. This is particularly a problem for small and rural hospitals, which do not make large profits on individual services that can offset the losses from reductions in the number of services delivered. These hospitals could be forced not just to eliminate services, but to close entirely.
Under a patient-centered payment system, most of the payments for hospital services would come from the hospital’s share of Acute Condition Episode Payments for procedures and treatments delivered in the hospital and payments for individual services delivered in the hospital for uncommon and complex conditions, and the amounts of these payments can be set at levels designed to cover the cost of delivering the services to the number and types of patients who need to receive services in a hospital. However, in addition to specific procedures and treatments, a hospital delivers an important set of services to the community that are not directly supported by current fee-for-service payment systems and that would not be adequately supported through the patient-centered payments for primary care or specialty care:
- Emergency Services. A hospital emergency department must be adequately staffed and equipped to handle rare events such as serious accidents, natural disasters, infectious disease outbreaks, etc., while also hoping that no such events actually occur. In addition, in a small commmunity, the emergency department must be staffed on a round-the-clock basis even though there may be few or no visits at certain times of the day, and it has to have adequate capacity to handle multiple visits at a time when they do occur. Providing this “standby capacity” is an important service that all of the residents of the community benefit from, but there are currently no payments explicitly designed to support it.
- Other Essential Standby Services. In addition to the emergency department, certain other hospital departments, such as a cardiac catheterization unit, a labor and delivery unit, a radiology department, a laboratory, and/or a surgery suite, must be staffed and ready to quickly respond to heart attacks, strokes, premature births and complications of labor, major trauma, sepsis, etc. on a round-the-clock basis even if some of those situations occur only occasionally, particularly in small communities. The hospital also needs a minimum level of inpatient care capacity so that it can admit patients who cannot safely be discharged home. Providers of ambulance services and specialized non-emergency transportation (such as wheelchair vans for disabled individuals) must have slack capacity in order to be available when needed. All of these services require that essential personnel and equipment are standing by in case a patient needs them, but fee-for-service systems have no payments explicitly designed to support this standby capacity.
Since there are currently no payments specifically designed to support standby capacity, the hospital or other provider has to cover the costs through the profits on other services it delivers. This encourages the delivery of unnecessary services and/or charging prices higher than costs. Not only are these strategies undesirable and often unsuccessful, they are even less feasible in a value-based payment system where primary care practices and specialty care providers are delivering care to patients outside of hospitals whenever appropriate. Consequently, a better way to pay for these standby services is needed.
Since standby services provide a benefit both to individuals who potentially need them as well as those who actually receive them, a patient-centered payment system needs to have a component to enable “potential patients” to support the standby capacity costs:
- Standby Capacity Payment for Essential Services. A hospital that provides essential standby services should receive a Standby Capacity Payment from each health insurance plan (Medicare, Medicaid, Medicare Advantage, and commercial insurance) based on the number of members of that plan who live in the community served by the hospital (regardless of whether the member receives a hospital service). The amounts of the payments should be designed to ensure that the hospital receives adequate revenues to support the minimum standby costs of essential services such as the emergency department, inpatient unit, and laboratory regardless of how many patients actually need services during any given month or year. Other providers that deliver services requiring significant standby capacity (such as ambulance services) should also receive Standby Capacity Payments designed to cover their minimum fixed costs.
If a hospital or other provider receives Standby Capacity Payments to cover the fixed cost of operating a service line, there would still be a need for an additional payment when a service is actually delivered in order to cover the variable or semi-variable costs of the service (i.e., the costs that are only incurred when an individual service is actually delivered, such as the administration of a drug). This payment should either come from an Acute Condition Episode Payment or a payment specifically for a specialized service. However, the amount of this per-service payment would be much lower than current fees for such services, since it would be based on the marginal cost per service (i.e., the magnitude of the variable cost component), not based on the average cost of the service as fee-for-service payments typically are today. This will help make essential hospital services more affordable for patients, particularly those without insurance.